
Introduction
The title of this post in the covid-19 series here is from a pamphlet by Lenin at the end of October 1917. Lenin begins with the words “Famine is Approaching”:
https://www.marxists.org/archive/lenin/works/1917/ichtci/index.htm
We are not in that situation nor anything like it. But there is an impending catastrophe which has been thoroughly documented by the “Imperial College Covid-19 response team” in a series of technical reports:
https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/news–wuhan-coronavirus/#
The current absurd floundering will not result in famine. But it could result in more avoidable deaths from Covid-19 than the total deaths from the “Spanish Flu” which killed more people than the “Geat War” that immediately preceded it – the “War to End All Wars”.
This is very likely in countries ruled by Kleptocracies like many in Africa. But already the failure to prepare is killing large numbers in Italy, with Spain and France close behind and London less than three weeks behind Italy on the same trajectory. Lots of people will also die unnecessarily in countries that are modern industrial democracies with blithering idiots in charge of pretending the owners care about the people.
The potential catastrophe we face is much smaller than the consequences of famine. A Case Fatality Rate of 6% or so instead of less than 1% that could have been achieved if quarantine arrangements were prepared to spread out the peak case load. Say half a million avoidable deaths in the UK, 2 or 3 million in the USA, less than a hundred thousand or so in Australia. Nowhere near as bad as famine…
Most of the deaths will be the result of hospital Intensive Care Units so overwhelmed they cannot provide life saving treatment for the most severe case numbers beyond available capacity.
Figure 3 of this recent authoritative announcement has a clearly labelled graph on “flattening the curve”:
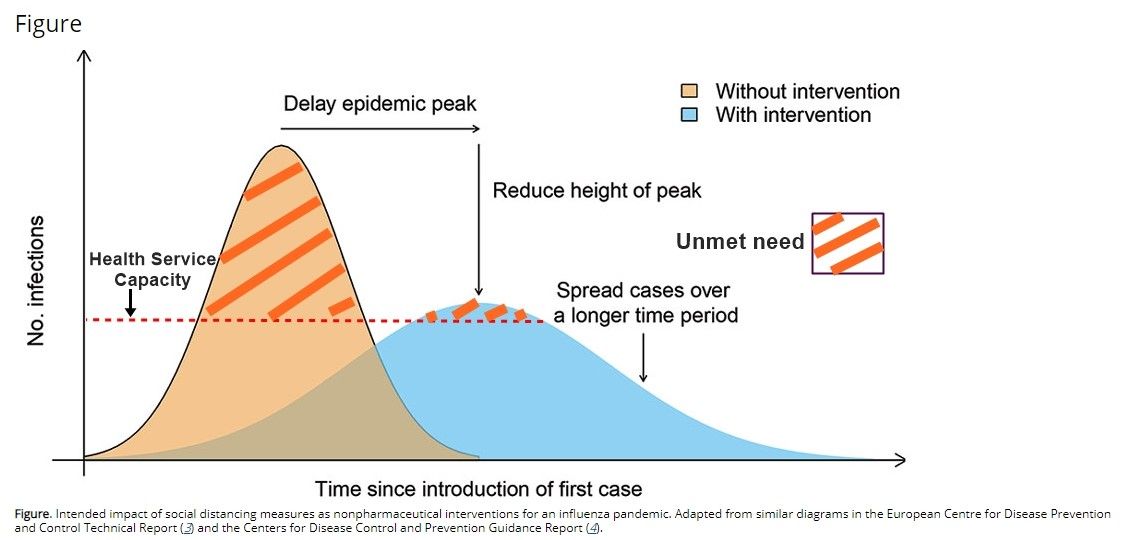
Instead of just the usual horizontal line showing “Health System Capacity” lower than an early high peak and just above a slower spread out peak it adds a label for the very large shaded region above that line for the high peak and the smaller region still above that line, for spreading out.
The label is “Unmet Need”.
That is clear enough. A sharper version, more easily understood and acted on would be:
“Avoidable DEATHS not prevented”.
But even the milder version is omitted from more recent authoritative announcements.
Australia is on roughly the same trajectory as London, Italy and the United States. “Community Transmission” is already well under way in NSW and Queensland and has just got started in Victoria. It makes sense for the other States and Territories to close their borders to buy some more time just as it made sense internationally.
But it won’t be enough.
Update: If this sounds alarmist check out today’s Australian on what others far more qualified to express an opinion are saying:
Infectious disease modellers say the current round of restrictions would quarter the number of likely infections at the peak of the epidemic, but even with those social distancing measures in place, unless further measures were taken, Australia could still hit a peak of 125,000 infections a day — a level that would overwhelm the nation’s intensive care units.
…
Cases of COVID-19 are currently doubling every four days in Australia and heading towards a trajectory of a three-day doubling. If the epidemic were allowed to continue in this manner, University of Melbourne epidemiologist Tony Blakely said infections could climb to as many as 500,000 a day within weeks.
Under that scenario, the reproductive number of the virus is 2.5 — meaning every person infected with the virus would pass it to 2½ others. Social distancing measures are likely to reduce the reproductive number, known as R0.
Professor Blakely has modelled the impact of social distancing measures and predicts the moves to close pubs, clubs, restaurants and sporting facilities could reduce the R0 to 1.2 by the end of May. That would see the epidemic peak at about 125,000 infections a day in late May, with 60 per cent of the population infected.
Based on modelling completed by epidemiologists from Imperial College London, and adapting their model to Australia, Professor Blakely predicts that by the epidemic’s end, 165,000 people, or 0.84 per cent of cases, would require intensive care, assuming 60 per cent of people of all ages were infected.
Medium Term
Below on “How to Combat It” is mainly about short term measures. Days and weeks of “Impending Catastrophe”.
Fortunately longer term measures are already under way as explained at the end
Scientists and “nerds” are already pushing aside the barriers to effective cooperation from “Intellectual Property” far more rapidly than the rest of society is moving to push aside other forms of private property in the means of production.
The Enlightenment “Republic of Letters” is emerging again in a modern form with rapid mobilization forcing changes in public health policy as documented in earlier articles of this series:
covid-19 Over 70s must self isolate for 4 months. Scientists demand immediate “social distancing”
Covid-19 – Don’t Panic – Do Self Isolate
For those who think they already understand and could not even bother to read the links in those posts there are already some excellent animated videos to explain the basics eg:
Why the actual numbers are much larger and growing faster than the statistics catching up:
Estimating actual COVID 19 cases (novel corona virus infections) in an area based on deaths
Some visualizations that are steps towards “Explorable Explanations” with sliders and other widgets to get a “feel” for what is happening and what can be changed can be found here:
https://observablehq.com/collection/@observablehq/coronavirus
Inceasing Healthcare Capacity
It also makes sense to immediately commandeer hotels as well as private hospitals for conversion into Emergency Hospitals and use entirely separate hospital buildings for covid-19 rather than attempting infection control within the same hospital buildings as wards for other patients. No doubt that will all be done along with many other things to raise capacity.
For those interested in the measures for rapidly expanding healthcare capacity a thorough current account of covid-19 for Emergency Medecine Critical Care professionals is here:
https://emcrit.org/ibcc/covid19/ (about 50pp as of 2 March)
Only the first section is likely to be of wider interest to other health workers. I think that first section is adequately summarized for a wider general audience in the public information campaigns now based on accurate advice from Centers for Disease Control etc. Note that the discussion of precautions against possible airborne transmission in above link is only relevant for those actually treating infectious patients.
No doubt surgeons no longer doing elective surgery will be taught how to do intubation procedures to provide ventilation for the vastly increased numbers of severe cases with viral pneumonia including many with further complications such as bacterial pneumonia, even though most of the teaching will be on the job assisting. Inferior split ventilators will be used and supplies will be ramped up.
Supply Chains
Naturally the main focus of the media has been on shopping. The newspapers are printed on the back of ads for shopping and the broadcast news is squeezed between ads for shopping both online and on air.
My view is that the shopping shambles is not of major signifcance and will be sorted out without major impact. Even if 80% of the workforce have mild to moderate illness lasting 2 to 3 weeks over the same relatively short period and there is disruption generally, essential services can be maintained. Most workers are employed to not do anything useful, let alone essential. Workers from large sectors shutting down now can be fairly rapidly mobilised as (unskilled and bewildered) assistants in essential areas while training on the job.
That is what I expect to happen when the blithering idiots in charge notice that funding businesses to continue trading while insolvent does not actually achieve much in the long term for a shutdown that reduces their turnover to near zero. Even the sheer idiocy of disrupting all credit arrangements by not enforcing payment terms so that deliveries will only be for cash will not be catastrophic in itself although the financial system may be fragile enough to come up with a related catastrophe.
Some fumbling and blunders are inevitable. The supply chains for groceries and pharmaceuticals will recover from panic buying without those stuff ups in emergency management causing many unnecessary deaths. The shortage of face masks and alcoholic sanitizers was avoidable but not necessarily catastrophic.
Impending Catastrophe
So what is the “Impending Catastrophe” if the Medium term is looking good, healthcare capacity can be rapidly expanded and supply chain hiccups are not especially catastrophic? Simply this.
There is no reasonable prospect of increasing the capacity of Intensive Care Units rapidly enough for a pandemic that will accelerate to double the case load every 2-3 days. A week after hospitals reach full capacity they will be dealing with a case load more than four times capacity. A fortnight later, more than 16 times. This is happening now in Italy. London is about 3 weeks behind Italy and Australia and the USA not much further behind, all on much the same trajectory that leads to catastrophe.
What cannot be fixed quickly enough for the first peak is the supply of mechanical ventilators etc for Intensive Care Units. Vastly accelerated scale up still cannot possibly keep pace as countries are now entering the period of doubled demand every 2-3 days:
Clin Infect Dis. 2015 May 1; 60(Suppl 1): S52–S57.
Published online 2015 Apr 10. doi: 10.1093/cid/civ089
Estimates of the Demand for Mechanical Ventilation in the United States During an Influenza Pandemic
Martin I. Meltzer,1 Anita Patel,2 Adebola Ajao,3 Scott V. Nystrom,4 and Lisa M. Koonin5
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4603361/
The impending catastrophe is lack of preparations for serious quarantine.
Given a shortage of Intensive Care Units and no vaccine, such measures are the ONLY way to prevent or reduce catastrophe.
Quarantine
The measures for people outside the health system to focus on are for “flattening the curve”. Spreading out the infection directly reduces the death rate by directly reducing the number of people with severe cases who cannot be treated when they all arrive at hospital Intensive Care Units at once and equipment is available for only a fraction of those who need it.
That is not something achieved by telling people to stay at home doing nothing. It requires actually building and organizing things.
We need to actively build and organize QUARANTINE facilities. This is not just passive “social distancing”.
The whole point of the “containment” phase of tracking new arrivals for a short period of “self-isolation” and closely tracking the contacts of anybody infected was only to buy time before “Community Transmission” began. Containment merely keeps the numbers of new infections “contained” at a smaller rate to delay the “local transmission” that will inevitably eventually grow at a much larger exponential rate until “herd immunity” is achieved with effective vaccination (expected 12-18 months away). Some cases were bound to get through and eventually result in enough people infected from unknown local contacts that the origin of most new infections is “the community” rather than some tracked or untracked individual cases seeded from outside. Then the pace accelerates from doubling each week to doubling each 2-3 days as in Italy and others that are near the first peak.
The World Health Organization, WHO, has recommended “test, test, test” because the surprise at the Italian hospital system being overwhelmed showed the pandemic was being fought blindfolded. Containment through border control and isolation cannot work when you do not know who to isolate from whom. It was known since late January that most people infected had only mild symtoms or none (with estimates of 86% of cases not reported in the statistics that media have been relentlessly staring at).
Even with an adequate supply of test kits there has to be somewhere to put people who test positive for the couple of weeks or so until most of them recover. Instead they are being told to stay at home and infect the rest of their household who are now (belatedly) being told to also stay at home. That will reduce the acceleration more than if they were told to just keep going out. But three very urgent measures were obviously necessary then.
Their necessity should have been announced loud and clear while rolling out implementation as fast as possible after announcement. So far not even the necessity has been announced. Here is my view of the three most urgent measures that are critically urgent now:
How to Combat It
1. Quarantine Hospitals for the mildly and moderately ill
Also separate facilities for unconfirmed suspected likely cases (eg travellers from areas with more community transmission to those with less).
I don’t know what the correct term is for what I have called “Quarantine Hospital”. People who don’t live by themselves should obviously not be told to just stay at home and infect their household while they wait to see if they are actually infected or while recovering. Nor should they occupy full hospital beds needed for people more severely ill.
The rest of their household can be told to just stay home for a couple of weeks to see if they are already infected or not, but anyone infected should be immediately separated from people who are not known to have been infected. That is blindingly obvious whether they need additonal medical treatment or not and whether any treatment they need is available or not. Any country not doing this is not seriously trying to flatten the curve.
“Quarantine Hospital” sounds better than “Quarantine barracks” but just somewhere to stay and be fed with some nursing staff is all it takes to seriously spread out a peak. It will require an enormous effort but it can be done using space that must be shut down anyway, emergency furnishings and staff from businesses that must be shut down anyway.
Commandeering hotels etc is for full emergency hospitals, not for the larger numbers of beds needed in Quarantine Field Hospitals. Lots of office space unused with people working from home and entertainment venues shut down must be converted to emergency accommodation. The kitchen facilities are available from the cafes and restaurants being shut down. The beds and bedding are available from households in proportion to the numbers moved out of households that will need those beds, and the staff are available from the huge numbers of small businesses trading while insolvent as well as from those already laid off. So far as I can see that has not even been planned, let alone started.
2. Quarantine Accommodation for the vulnerable
Older people and people with various severe health probems are especially vulnerable to being part of the less than 1% who might die before a vaccine is available or part of the additional 5% or so that are killed by government incompetence as a result of intensive care not being available for them when the hospitals are overwhelmed. No doubt local communities will get organized to help those who need help while staying isolated in their own homes but there are others staying in households with less vulnerable people equally susceptible to infection.
“Tough” restrictions on visits to aged care institutions are obviously ludicrous. These can only be intended as justification for very soon saying people had an opportunity to make their last visits immediately before an essential full shutdown until proper procedures for safe visits fully separated by glass barriers etc can be organized.
But vulnerable people currently living in households with others must also be offered accommodation separated from the rest of the susceptible population until the peak has passed and sufficient intensive care facilities are available. That will be hard for many. Many may refuse and many may die. But doing nothing to make viable separate accommodation available is criminal. That seems to be the current “plan”.
Neighborhood support groups are starting to be formed spontaneously through social media:
https://www.abc.net.au/news/science/2020-03-17/coronavirus-online-support-groups/12060530
It is important to keep them entirely separate (although overlapping with) closed small “affinity” groups of households with children discussed in item 3 below.
3. Quarantine Separation of children
Obviously schools will have to be shut at some point except for children of households working in healthcare and other essential activities. Meanwhile schools are vitally important community organizing centers for households with children.
The shutdown won’t just be for a couple of weeks. It will end up lasting for many months.
while still open, and even after closing, schools should be organizing children into small groups, much smaller than class sizes, that will be allowed to interact with each other within school and after the shutdown and prohibited from doing so between groups.
This obviously needs to be coordinated with parents because all the households with children in whatever group any child continues to interact with will tend to get infected together. It will be especially difficult for households with children in different age groups and different schools but every household with children must be assigned to a particular group of households it is permitted (not required) to socially interact with. The kids are not going to just stay at home with their parents for six months, let alone eighteen months! Humans evolved in Hominid bands of a couple of dozen, not as isolated nuclear families.
Hopefully if we move really fast the necessary interaction can be online in Virtual Reality but we don’t know how well that will work, for how long or how quickly. It still ought to be based on non-overlapping groups that should be organized now by schools.
These separate child based groups are likely to continue to mix with and infect each other and must accept that their own group of households will or may end up having the larger risk of earlier infection corresponding to an enlarged single household. They must be confined to small numbers of households who trust each other to maintain isolation from the rest of the world to the same extent as the individual households.
Households with older and more vulnerable people are a major complication as self-isolation within a household is unlikely to be effective for long.
Six months is a rather optimistic estimate of how long this crisis will last. It could “conceivably” be as short as 6 months if all goes perfectly but that is not the period to plan for now. Avoiding overwhelmed hospitals requires dragging things out longer, until an effective vaccine gives “herd” immunity or effective anti-viral drugs reduce the death rate. Even if it could theoretically be even shorter than six months most serious estimates are for 12-18 months of on and off waves.
The current authoritative recommendations are that it is still too early for school closing in Australia:
https://www.health.gov.au/news/australian-health-protection-principal-committee-ahppc-coronavirus-covid-19-statement-on-22-march-2020
But that is based on lack of positive evidence that the time is right. See below on tests.
Evidence
Evidence in support of much of the three proposals above can be found from the experience of South Korea so far:
But even Italy where the hospital overload is currently greatest has only had 0.1% of the population as “cases”.
South Korea has a very long way to go before herd immunity and there is nothing in the lower numbers of new cases after the first peak or the success in dealing with that first peak to suggest that there won’t be many further peaks:
https://www.worldometers.info/coronavirus/country/south-korea/
Likewise for Singapore, another success being hailed as though it were not just success with the first peak.
I don’t know whether anybody has solid evidence of whether and how it may be possible to stop transmission between househods via their children during an extended shutdown. As far as I can make out there is just empty hoping that for some unexplained reason it won’t happen. This mainly takes the form of highlighting the distraction that children have much less severe symptoms (which actually enhances their role as disease vectors).
Current Plans
Compared to Australia and the USA the UK is a model of serious but still unsuccessful efforts to explain public health policy to the public via journalists in a joint effort by the PM, the Chief Science Officer and the Chief Medical Oficer.
It is worth spending the time on these two long videos less than 5 days apart to understand how rapidly the situation is changing and how uncomprehending the journalists covering the “issue” are.
Coronavirus: Boris Johnson holds press conference after Cobra meeting
308,797 views – Streamed live on Mar 12, 2020 – starts at 23’30” of 1:10’57”
Coronavirus: Boris Johnson sets out “drastic action” BBC
292,849 views – Streamed live (Mar 16, 2020)
The pandemic model that now forms the basis for planning in the UK expects multiple waves of infection each time “social distancing” is relaxed after successfully suppressing the peak rates to reduce case loads to hospital capacities. This is in Report 9 from the Imperial College team:
https://time.com/5804555/coronavirus-lockdown-uk/
A shorter Australian attempt at explaining the model to a journalist is this video from the ABC’s Dr Norman Swan on 17 March. (I watched it after having written the rest of this article). In many ways it is better than the UK and Australian official explanations but he still ends up distracted by issues of case tracking from the “Containment” phase rather than the current accelerating exponential growth on entering the “Community Transmission” phase. He simply does not get the fact that spreading out the peak necessarily reduces total deaths from unavailable intensive health care units and instead claims that a spread out peak could still have the same total deaths.
“Explorable Explanations” with widgets for people to actually manipulate the paramaters of the models themselves are really essential instead of literally hand-waving – with or without a background graph:
If any of these people trying to explain had access to such Explorables they would be using them on TV. Instead they are waving their hands.
The primary mechanism for transmission during a long shutdown might well be the overlap between different groups of children from different groups of households interacting to transmit the virus between their otherwise separated groups of households. It will certainly occur with younger children still at school.
Similar transmission will occur from the essential workforce in different workplaces also transmitting between different households, but stringent “social distancing” controls at work can reduce that far more effectively than among younger school children. Likewise smaller households without children will get infected more slowly than extended groups of households whose children infect each other.
Tests
School closure timing and arrangements is the hardest issue to grapple with and the least data is available as to transmission rates through these channels. Currently there have been no adequate systematic random samples of the population generally as test kits are only available for more urgent needs such as border control during the containment period and testing health workers.
In particular there is no blood testing yet to measure the immune system responses of people who have already had the virus without symptoms. Such testing is hoped for soon and could be a game changer for enabling decisions on the optimal timing for imposing and lifting isolation restrictions before and after hospitals are overloaded. It could also shed a lot more light on the transmission between children and between adults and children. At present decisions on how to time for less overloading of peak capacity in successive waves are being taken blindfolded.
The separation of groups of children and their households necessarily involves the widest participation in community decision making and implementation and the most discussion to come up with ideas right now. Explorable explanations with widgets are needed urgently for this.
All UK schools closed last week, very shortly after official announcements that the best “science” showed that overall effects of closing schools could be negative because of:
- Large effect on essential workforce diverted back into parenting and child-minding, especially from already overloaded health system. (Private schools closed earlier but essential workforce is generally lower paid with a high proportion depending on schools for childcare while working in health system).
- Likelihood that traditional reliance on grandparents to assist will result in more rapid infection of the most vulnerable.
- Unlikelihood that school students will remain socially distanced from each other while away from school, short, medium and long term.
Previous announcements were correct. So is the new decision.
What follows from the correctness of the two opposite decisions of our dearly beloved leaders both 5 days earlier and 5 days later is that urgent mitigation measures can and should be taken for all 3 issues. Others can contribute more to discussion of those measures so I won’t attempt it in this article.
All I can say on it is that school closures will happen soon whether desirable or not.
Here is some confusing advice from USA of the same sort that will dominate discussion here:
In addition to the advice only now being widely disseminated by authoritative public health information campaigns, households with both children and older and more vulnerable people should carefully consider stronger advice from people who have been campaigning for full social isolation to be implemented sooner.
https://www.endcoronavirus.org/
They also have an interesting critique of the mainstream epidemiological models:
https://static1.squarespace.com/static/5b68a4e4a2772c2a206180a1/t/5e70eb32b16229792eb14836/1584458547530/ReviewOfFergusson.pdf
They cannot be considered “authoritative” but I will be carefully studying the technical background necessary to be able to understand both.
Epidemiology for the Uninitiated
Lots of people, like me, will need to acquire some basic epidemiological concepts to understand what the models are about. Studying this is very good practice for understanding the economics of the capitalist business cycle. (The Explorable Explanations will be more accessible for most people both for pandemics and for the business cycle).
I will be starting here:
https://www.nature.com/articles/nrmicro1845
Book chapters: https://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated
Another critique of earlier UK (and current Australian) policy is here:
https://unherd.com/2020/03/the-scientific-case-against-herd-immunity/
If the serious critics are right there won’t be another peak in China and Italy after full social isolation measures are enforced. If the mainstream epidemiological view is correct (as opposed to the government waffle about 6 months) there will be successive waves over 18 months or so until a vaccine is effective, possibly ameliorated by anti-viral drugs. This is because “social distancing” restrictions end up becoming intolerable and therefore ineffective and get relaxed because they cannot be maintained for long when new cases decline to near zero after dealing with each peak in the overloading of ICUs and consequent deaths from unavailable medical treatment. Transmission can be expected to resume gradually and then again suddenly as long as there are large reservoirs of people still susceptible. There will still be large reservoirs susceptible to infection after the first peak overloading the hospitals is shutdown by emergency isolation measures just as there was for the first peak.
The business press is already editorializing about not “over reacting” and the importance of quickly getting people back to work for them. Their views will eventually prevail while the owners are still in charge. Here’s a couple of the Wall Street Journal’s editorials urging that more people be killed quickly to save money:
https://www.wsj.com/articles/rethinking-the-coronavirus-shutdown-11584659154
https://www.wsj.com/articles/the-extreme-state-lockdowns-11584745130
They can rely on help from lots of people who think correct ideas fall from the sky or are inherent in their minds as “just common sense” and are simply not interested in studying the knowledge acquired from social practice and from it alone. The three kinds of social practice include class struggle, the struggle for production and scientific experiment. This is not a good time to be glued to the business channels and ignoring the political class struggle and the struggle for production being waged by workers in the relevant sciences.
Simply assuming the first peak will be the last is as helpful as the Wall Street Journal’s editorials.
The kind of mathematical modeling that is done to help inform public health policy for dealing with this pandemic is closely related to the sort that is needed for understanding the capitalist cycle and the transition from capitalism. So studying the pandemic is not a diversion from other priorities.
Long Term – the “Republic of Letters”
https://en.wikipedia.org/wiki/Republic_of_Letters
The modern form of the “Republic of Letters” is very much based on the communist mode of production and distribution already widespread in the Open Culture (eg Wikipedia) and Open Science offspring of the Free and Open Source Software movement. Such intellectual activity was not enough to produce the Enlightenment, let alone the bourgeois democratic revolution against Feudalism. Nevertheless it was a very important precursor.
Wikipedia has an impressive portal showing the current extent of collaborative effort:
https://en.wikipedia.org/wiki/Portal:Coronavirus_disease_2019
The “pirate” backbone for disseminating scientific and other knowledge from “Library Genesis” and “Sci-Hub” is being hardened against attack and is openly confronting the crisis:
The main scientific publishers have accepted demands to make all covid-19 research immediately open access (they were being bypassed anyway by pre-prints on community archive sites and by Sci-Hub).
Activists have organized collections of relevant non-current background material. Major Big Tech companies have co-opted the US government to neatly classify what is “Open Access” and what needs to be extracted from behind paywalls and disseminated by activists:
https://pages.semanticscholar.org/coronavirus-research
COVID-19 Open Research Dataset (CORD-19). 2020. Version 2020-03-13. Retrieved from https://pages.semanticscholar.org/coronavirus-research. Accessed YYYY-MM-DD. doi:10.5281/zenodo.3715506
Game players with fast Graphics on home PCs are being enlisted for anti-viral drug research:
They have vastly more potential computing power than Big Government and Big Data combined:
The 34,000 GPUs mentioned in that article are a drop in the ocean compared to what mobilizing the gamer PCs can deliver.
So anti-viral drugs and vaccines will arrive a lot quicker than usual, as will saner public health policy.
Even before governments started using their powers to commandeer manufacturing resources for ventilators and other hospital supplies, people started organizing to just do it:
As already mentioned, the Emergency Medecine Critical Care professionals took care well in advance to prepare training materials for their reinforcements before they are overwhelmed:
https://en.wikipedia.org/wiki/EMCrit
A semi-random example of the sort of highly skilled know-how that will need to be increased with extreme acceleration is:
Its interesting that a couple of possibly relevant books listed there have later editions at Library Genesis than the editions mentioned:
Tobin, Principles and Practice of Mechanical Ventilation, 3edn (1500pp)
http://gen.lib.rus.ec/book/index.php?md5=F1730DC52D2BF1A73E857691AF3858FF
The Walls Manual of Emergency Airway Management, 5edn
http://gen.lib.rus.ec/book/index.php?md5=BFA1F68808415E2FA52607AA3F17.
Unfortunately Library Genesis does not have the only book in that list with the word “Intubation” in the title, nor any others in english that look relevant:
The Airway Cam Guide to Intubation and Practical Emergency Airway Management 1st Edition, Richard M. Levitan
Presumably anything relevant wih a doi can be obtained via Sci-Hub or this can rapidly and easily be arranged by the relevant professionals if necessary. Activists are working now to make the relevant materials freely available for people who will find themselves on the front lines along with other health workers quite soon.
Anyway, people are moving way faster than governments.
A new world is being born from the ashes of the old.
Bulk Edit

Arthur2 minutes agoUser InfoIn reply to:[…] https://c21stleft.com/2020/03/13/covid-19-dont-panic-do-self-isolate/ […]
Update: Today’s Australian (Tuesday 2020-03-24) also has confirmation from Singapore PM that further waves are expected. I did not notice it last night:
“We are under no illusions that the problem is over at all,” he says.
“If I made an analogy, it is not that the tide has turned, it is that we put the dykes up. We are watching very carefully to see where water may leak in, and if you take your eyes off it for a moment, suddenly I have an outbreak, like what happened in South Korea, and I will be in a perilous situation. It can happen to us at any time.
“Australia is grappling with the same problem. The countries around us in Southeast Asia are also facing the problem. It (the outbreak) is going to catch fire in many countries and is going to take a long time to burn out.”
…
“I would not say we have successfully prevented it,” Lee says carefully. “I think I would say so far we have reasonably successfully hindered the transmission.”
The key, Lee explains, is checking out all the people any infected person may have unwittingly infected before diagnosis.
“We work very hard to contact-trace,” he says. “Who are the people you have met within the last two weeks, where have you been, what have you done, who may have been exposed to you?
“We make every effort to trace those people down as well and put the immediate contacts either on notice or in quarantine, depending on whether they have symptoms. It is very labour-intensive. We have 300-plus cases now, but we have contact-traced several thousand people already, at least.
“It is labour-intensive but it is helpful in preventing a single case from becoming many hundreds of cases, if you catch it in time.”
…
“Looking at the behaviour of the disease and the way it is jumping from country to country, you can push it down within a country, but it has not disappeared worldwide,” he says.
“I think this is going to be with us for quite some time.”
…
“Their population is not immune to it yet, in very large numbers. Because even if a million Chinese have got the virus so far, that still leaves almost 1.4 billion people who have not yet, and are still, in immunological terms, naive and at risk.
“So, what you can hope for is that you control the spread of the disease, you hold the position, and hope and pray that the scientists come up with either a treatment or a vaccine within a year or two — and in time for us to exit this without the doomsday scenario, namely that the disease goes through the whole population, and then eventually we have herd immunity. Either it is going to leave you with huge casualties, or it is going to take forever to lock down.
“I think it is an enormous economic cost, and a human cost too.”
Note: Like South Korea the proportion of the population that remains susceptible to infection in the next wave is even higher than in China where one province, Hubei did have an initially uncontrolled outbreak so are substantial proportion of that province now does have at least short term immunity so there is a fair chance the next wave there will be smaller.
The proportion still fully susceptible in Singapore and South Korea is as close to 100% as makes no difference. So whether the next outbreak is smaller or larger depends largeely on how effectively long term “social distancing” can be maintained until a vaccine. The initial success was “containment” using tracking and quarantine. When actual “Community Transmission” develops rigorous quarantine becomes far more important as then tracking merely confirms that most of the new cases were infected from “the community” rather than from a specific known contact who can be promptly isolated.
Unlike any other statements I have seen from national governments Singapore is clearly stating what the media and pretty well everyone who thinks they don’t need to know more, does not yet understand.
But it still needs “Explorable Explanations” of the model for even a small minority to not be surprised when subsequent waves happen.
[Tried to add this update as a comment but will have to figure that out later]
