Update 6: Tuesday 2020-Apr-14 T11 am
All’s well. Got call that this story is also in “The Age”:
“Patients with COVID-19 could be quarantined in ‘medi-hotels’ instead of at home in a bid to prevent family members and housemates from being infected and ensuring compliance with isolation requirements.
Federal Health Minister Greg Hunt he was “very open” to the medi-hotel concept, which is being trialled in Tasmania at the behest of the state’s peak medical body and is based on the Singapore government’s approach.
…[more]…
Will still work on some submissions about it but can relax now and setup laptop and also do other work and write about other stuff.
Update 5: Tuesday 2020-Apr-14 T02:30a
The figures really needed is the daily new additions to “community transmission” (“locally acquired – unknown”).
Growth rate R_t for that is critical. Determined by lagged total infections and ratio of net new infections (including lagged “under investigation”) that are from unknown source of local transmission.
Guardian compiles its own up to date spreadsheet here from States and Territories:
https://docs.google.com/spreadsheets/d/1q5gdePANXci8enuiS4oHUJxcxC13d6bjMRSicakychE/htmlview#gid=0
https://www.theguardian.com/australia-news/datablog/ng-interactive/2020/apr/13/coronavirus-cases-australia-numbers-new-stats-graph-map-by-postcode-covid-19-death-toll
Guardian also links to a Google Docs spreadsheet of daily new cases by jurisdiction in 5 categories of source (including interstate)
Need additional breakdown of daily movements from “Under investigation” to each of the other categories or at least to “locally acquired – unknown” ie “community transmission”. From that can calculate lag on “Under investigation” to eventual “community transmission” for a more accurate estimate of trend in new additions to community transmission.
But numbers seem to be around 10 and so would need a few weeks to distinguish clear trend from noise.
https://docs.google.com/spreadsheets/d/115_BZLlrGcXcTU_Ogtl38BMr1yKKrXPSRr6JpPeSnME/htmlview
Need link to most recent versions and related background info.
“Please email nick.evershed@theguardian.com or australia.coronatracking@theguardian.com with suggestions or errors.”
Ask them for URLs to more raw data and/or help ask for additional above.
Update 4: Sunday 2020-Apr-12 21:30 pm
Current figures indicate that the number of new cases each day is stable or “flat” at around 100 per day from 5 to 10 April.
This has resulted in talk of being on the “cusp” of success with pressure to start planning for “exit” from restrictions, together with cautionary warnings from epidemiologists that we won’t actually know for a couple of weeks since data on “community transmission” is currently mixed together with data from overseas acquired cases and the different effects of recent measures on those two categories will not become clear immediately.
Either side might be right. Nothing is certain.
But my view is that both sides are wrong. To me the fact that the numbers look more or less flat at the moment almost necessarily implies that we are currently at the bottom of a sharp decline in the transmission rate that will be followed by a rise. A flat period is what you get at the bottom of a trough (as you do at the top of a peak).
Two measures were taken almost simultaneously.
- Incoming travellers enforced quarantine from midnite Saturday 28 March.
- Major increase in the level of “social distancing” with decision for 2 person limit on social gatherings Sunday 29 March (enforced by States over next few days).
At the time it was stressed by the committee of Chief Medical Officers in charge that:
“…there is a lag time of at least 7-14 days before the real impact of additional measures will be seen on case incidence, and longer for critical care requirements and mortality”.
But less than two weeks later, many people actually believe they can already see the real impact because the numbers look flat to them.
If the numbers are as flat as they look that is actually a strong indication that the measures are not sufficient to prevent community transmission continuing to grow exponentially rather than beginning to decline exponentially or remaining flat.
Certainly with the current levels of “social distancing”, the positive exponential growth rate will be much slower than the catastrophic doubling twice a week that occurred immediately after the daily new cases first reached the present flat level of around 100. That was the same trajectory as the overwhelming of hospitals in Italy, Spain, UK and USA which led to sudden imposition of essentially the current measures here in Australia (and much stronger measures in New Zealand).
But it is logical to assume there will be continued exponential growth at a slower rate because at present a sharp rate of decline in transmission from the large majority of new cases that were being acquired from overseas is being roughly balanced by the positive rate of growth in the small proportion of “community transmission” (less than 10% of total cases).
There are certainly grounds for optimism that this rate will be slow enough for further measures to succeed in preventing the hospital system being overwhelmed. But there is no basis for imagining that the figures do not ALREADY indicate that further measures are likely to be required, rather than providing grounds for speculating about “exit plans”.
Any rate of exponential growth at all necessarily happens first gradually and then suddenly. The decline in cases acquired from overseas will first be gradual and then sudden until they are an insignificant minority of cases. Likewise the growth in “community transmission” will first be gradual and then be sudden until what is now less than 10% of cases becomes the overwhelming majority.
That is simply too difficult for journalists to understand themselves, let alone explain to the general public. Nor can they understand that there will necessarily be subsequent waves after the first peak, since the large majority of people will not have been infected and therefore will still have no immunity until a vaccine at least 12 to 18 months away.
It requires “Explorable Explanations” with widgets so that people can “feel” for themselves what happens as you vary different parameters.
At present careful tracking of each case to determine the date of infection and the individual contact that caused infection is still feasible in Australia.
As at Saturday 2020-04-11 results are:
6,292 cases tracked of which the proportions acquired from different categories is approx:
- 65% overseas from a known contact (previously including tourists, students etc new additions mainly returning Australian residents).
- 24% local transmission from a known contact (mainly from known overseas acquired cases but also from other known locally acquired)
Both the above categories are controlled by tracking and isolating contacts of the previous source of transmission as well as contacts of the particular case. Only a small proportion of contacts of known cases are not successfully isolated. These together with the unknown numbers of people infected who never become known as cases because they have no symptoms that result in being classified as a case result in the additional categories below.
- 9% “community transmission” from an unknown local contact whose other contacts cannot be tracked and isolated. Only the subsequent contacts can be tracked and isolated so the rate of transmission is inherently much higher than from the fully tracked categories above. But the numbers are initially small.
- 2% “under investigation” as at 3pm on each date of reporting. Eventually each of these cases becomes one of the other three categories above. Those that do not become “overseas” or “local” end up classified as “community” when the attempt to track the original contact that resulted infection fails to identify anyone in particular whose contacts could then be tracked and isolated.
The new additions from overseas have been dramatically curtailed to an actual decline of less than 1 new infection per each arrival isolated under guard in a hotel room for 14 days. Otherwise there would not have been a sharp decline in total new infections each day.
Existing tracked local transmission and untracked “community transmission” has been substantially reduced because of greater “social distancing”. But that substantial reduction is not likely to result in less than 1 new infection from each existing infection. If it did then the overall result would be a continuing decline, not a “balance”.
When you see a pendulum travelling horizontally at the bottom of its swing, expect it to start rising unless further measures are taken to restrain it.
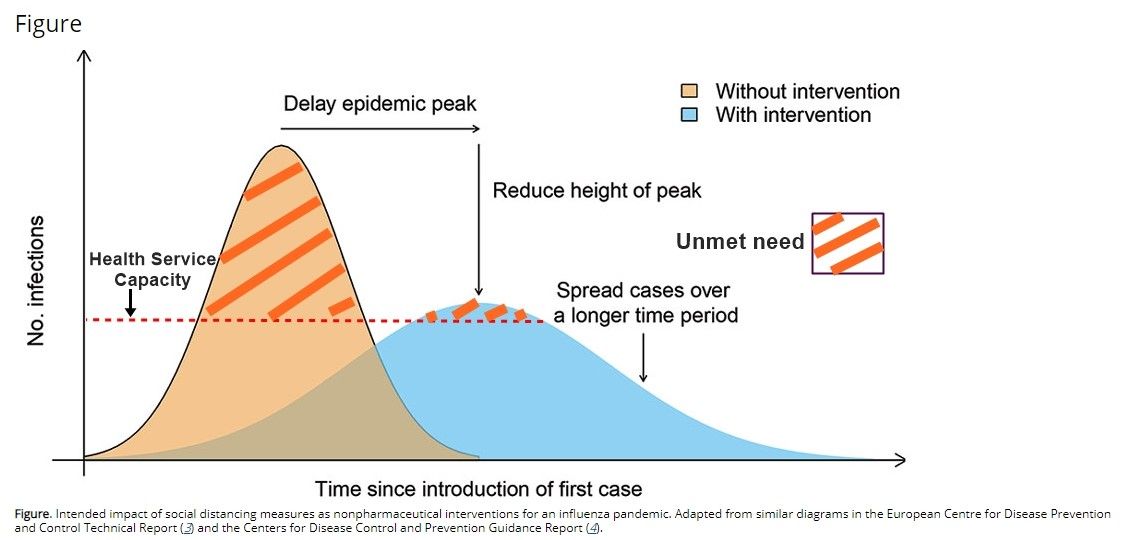
I expect those further measures to be taken. That could result in a “reasonable worst case” of the peak being delayed and limited so that it is within the capability of the hospital system to not be overwhelmed. Maintaining restrictions at the level required to prevent that growing could result in a prolonged peak with far more cases than now under far more restrictions than now.
That is called “flattening the curve”. It is a “reasonable worst case”.
That is what the public should be preparing for. In particular it will need a large roll out of short term quarantine isolation accommodation for both new cases and their contacts to help avoid the transmission rate rising to overwhelm the hospitals.
Further reductions in the death rate will also require long term quarantine isolation accommodation for vulnerable people living together with essential workers etc.
Update 3: Wednesday 2020-Apr-08 11 am
Very important guidance on Home Isolation from AHPCC. Study this carefully. Clear medical criteria that will necessarily require extensive rollout of accommodation (but not their function to organize that).
Also a separate government web page now has all links to the actual models of theoretical scenarios that simply confirm ICU capacity would be overwhelmed without measures already taken and might not be if those measures do work sufficiently:
https://www.health.gov.au/news/modelling-how-covid-19-could-affect-australia
Also has PM transcript:
https://www.pm.gov.au/media/update-coronavirus-measures-070420
As well as papers on the actual models the Doherty Institute page includes a short video with explanations from the two lead authors that should also be studied carefully. If anyone can get a transcript from the closed captions please do provide it. I don’t have time but it is worth quoting. Ends with:
Doherty Institute modelers are “now in transition from scenario analysis to data science driven situational awareness”
https://youtu.be/rhNrhGMog38
via https://www.doherty.edu.au/news-events/news/covid-19-modelling-papers (which also links two papers)
The above links are central to any work related to the post below and greatly simplify what needs to be said and done. Work towards preparing documents to persuading relevant people to say and do it will be at (and figure out how to reach the right people) will be done at link below. Please help there:
https://github.com/dentarthur/next-waves
Update 1: Tuesday 2020-Apr-07 17:25
I just read the two files released as “Australian government models”:
Even the media will quickly grasp that the Australian government simply does not have any local modeling capability and is being advised by people working blindfolded on their basis of models for vaccine controlled pandemic influenza.
Despite relying almost entirely on international models, such as those from Imperial College response team and belatedly drawing basically correct conclusions from those models (much slower than New Zealand) they have not even grasped the fact that there will be multiple waves and are primarily focussed on boasting about how well they are doing and how important the models will be. Its grim reading. Don’t worry about it being too technical to read. It is PURELY intended as a PR exercise with a derisory appendix with “parameters” on last page. Read it now.
Best hope for improvements is to bypass them via States and New Zealand.
Update 2 T20:15: Actually the Doherty Institute did release some modeling papers. The government web site URL just did not include any link to it but only some PR bullshit.
Here is the actual model:
https://www.doherty.edu.au/news-events/news/covid-19-modelling-papers
It does show an actual attempt rather than the derisary stuff above. I am still studying it but I would now say it is nowhere near the level of serious modelling as from Imperial College rather than being pure PR bullshit as above.
But it doesn’t look far beyond what anybody could produce by just feeding parameters into a web page and in particular this web page below which is a simple SEIR model at about the same level of sophistication and as distant from serious microsimulation and/or agent based modelling on HPC GPU clusters.
Situation still grim. But my guess now is that the Doherty Institute was asked to model ICU and other hospital capacity and the actual epidemiologists working with the public health authorities on current data simply don’t have time to chat with them about stuff for government media releases. There must be others working with better models.
Original post below:
I just watched the latest Four Corners. It did successfully highlight dangers that were obvious a full month ago and calls for actions that were needed earlier than that. But it rigidly avoided looking to the future and discussing the measures that are needed now and are still not being announced and prepared. Instead it repeated most of the actual video footage at least 3 times each. At one point I had to check whether I was watching a repeat loop of the video. They repeated exactly the same thing so many times to emphasize how little they had to contribute to actual thinking. But it is certainly worth watching to understand the state of public consciousness in Australia:
As far as I know the only places that may have got their initial outbreaks under temporary control are those that did move infected people to quarantine accommodation until 80% recovered from mild or moderate illness while not passing on infection and the other 20% or so became more severely ill and needed transfer to emergency hospitals. Since many cases are unreported with very mild or no symptoms they still initially lost control but recovered faster. These are Asian economies – China, Taiwan, Singapore, South Korea – with experience from SARS and MERS and very different social conditions to Anglosphere countries – Australia, NZ, Canada, US and the UK
By now other countries on the same trajectory to catastrophe as Italy and Spain should have at least announced an intention to follow the successful examples as rapidly as they can in order to avoid the looming catastrophe already occurring in some countries which did not. Instead Dr Birx, US coronavirus coordinator has announced that the US learned much from China’s experience as well as the UK Imperial College models, but that this Chinese approach of quarantine accommodation for people infected is not being followed. Instead of home self-isolation is more appropriate to American social conditions. The US and UK, like Australia are of course now adopting other, even more urgent, emergency measures for “social distancing” etc.
The conditions are different. Those Asian societies all have more crowded accommodation in which self isolation in homes shared with others not yet known to be infected is less feasible and a culture in which people are more likely to comply quickly with intrusive government health directions.
But those are grounds for careful preparation and rollout, which requires early announcement and offering the option of separate accommodation first on a rationed basis for those most likely to need it (including in the package of measures to maintain contact with households, school children and people especially vulnerable, to support mental health and coping generally). There should be announcements now about how to apply for such accommodation and apologies that it may have to be initially limited.
An obvious consequence of the different culture in countries like Australia is that it is far better to have people clamouring to be accommodated in quarantine than threatening them with compulsory quarantine (even if the latter also becomes necessary later). Therefore early announcements of not having the facilities ready yet are all the more important.
That would set the scene for rapidly ramping up the logistics operation currently dealing with a couple of thousand people returning to Australia each day and moving them to the larger hotels. That stream will dry up fairly soon but the capacity to handle accommodation for 50,000 cases and to increase it at 2000 per day will have been established in about two weeks and should be able to provide an “officer and NCO corps” for a larger mobilization following immediately.
The new stream of much larger numbers of people infected for a couple of weeks may soon completely dwarf incoming travellers in both numbers and significance.
Since so many activities have been shutdown, there is a much larger workforce available and lots of space available to roll-out whatever is needed. But it does take time to ramp up. Instead of just telling people to stay home to “fight the war” they should be told how to “sign up”. If a real mobilization will be ramped up over the next few weeks there should be announcements already and discussion about it even among people as detached from reality as ABC journalists.
On the positive side, at least Four Corners was not still twittering about such totally irrelevant issues as toilet paper panic buying and the relatively minor incompetence in managing supply chains for groceries and pharmaceuticals. The focus now is on the actual impending catastrophe rather than trivia that in any developed country will be quickly resolved and is unlikely to become a central cause of death even in poorer countries. Even if 10% of the population anywhere dies suddenly, essential services can and will be restored and maintained with any problems doing so being insignificant relative to the actual underlying catastrophe.
But Four Corners interviewed nobody about ANY measure that has not ALREADY been announced.
It was a “no-brainer” to point out that strict quarantine for 14 days should be enforced for anyone arriving from places with higher levels of community transmission and any contacts with people already infected. That has just been done. Most transmissions are still being seeded from international arrivals and tracking and isolation is still effective for more than half of all known cases. So it makes sense to do that before other things.
Likewise it makes total sense for those arrivals and other contacts who appear likely to be already infected to be isolated separately from others who are only being isolated as a precaution (whether those assumed to be infected are confirmed by test or not).
It does not require much in the way of brains to understand that with community transmission already under way in the largest three States everyone is currently “arriving” from a place with a higher rate of transmission (mixing with others outside) to a place with a lower rate (“stay at home”).
It equally makes sense to isolate as many as possible of those actually infected or assumed to be infected who are now being told to self isolate at home in separate accommodation rather than infecting the rest of their household who are also required to isolate in order to avoid spreading that infection to other households.
But there was no discussion of that at all. Nor have I seen any elsewhere.
I am sure the models would confirm that it is a much lower priority than measures that have been taken (belatedly) so far. That lower priority is because even if it could make a 100% difference between infection of 1 person and infection of 4 (which is far more than it could achieve), that is only a “once off” equivalent to one week of the recent rate of doubling. It is not an ongoing reduction in the rate and other measures were more urgent for achieving that.
But those remaining gaps and measures not yet taken to delay and lower the peak hitting the hospitals very soon are precisely what attention should be given to. Not the past or the more distant future.
Where are we now?
Worldwide it is still an impending health catastrophe developing into an ongoing current health catastrophe, especially for poor countries. Australia is several weeks behind Italy which is still in full catastrophe. A major campaign is being waged worldwide by the Wall Street Journal, assisted here by The Australian, for a more “proportionate” and “balanced” approach that trades off the number of avoidable deaths against avoidable damage to the economy. This “pro-death” campaign accelerates both health and economic catastrophe and is assisted by the rigid fixation of the rest of the media on breathless twittering about the past and the almost equally rigid fixation of actual decision makers on the “evidence based” present, both medical and financial.
Emergency Management in a pandemic is not about the past, nor the present but about the immediate future – the “future present” or “present future”. Triage of planning resources in an exponential period means the present has already passed and cannot benefit from planning.
Unlike normal affairs in which events occur at certain rates whose variability and response to interventions is within the understanding and experience of decision makers, an infection that doubles every few days is the future happening right now. The future happens in the present “first gradually, then suddenly”. It is what one has to orient to as happening right now from observation of the “road runner” cartoons running off a cliff with one’s legs rotating rapidly. Collecting evidence about the initial rate of descent and the distance to the cliff edge is a cartoon staple for illustrating a ludicrous lack of orientation even for quadratic descent under gravitational acceleration. The initial exponential period of community transmission happens much more suddenly than falling off a cliff after the earlier seeding happened “gradually” with all attention trained on daily numbers.
Given that the response eventually requires a full shutdown of non-essential activities while maintaining essential activities and intensifying emergency activities, the intertwining of health and economic measures necessarily requires war-time state capitalism rather than “stimulus”. It isn’t possible to make sense of what various governments and others are doing economically in the meantime so I am not attempting to.
What started gradually and was responded to by reassuring messages to the public that everything was under control (together with some measures to bring it under control) rapidly turned into something happening “suddenly” well inside the observation-orientation-decision-action loop of the decision makers responding to it so that they simply cannot prepare for what has already become inevitable. A pandemic is not an intelligent opponent to be taken by surprise. But it moves faster than decision makers can observe and then orientate before reaching a decision to take an action.
https://en.m.wikipedia.org/wiki/OODA_loop
Those of us who do not face the awesome responsibility of firefighting the current situation and being accountable for life and death decisions, can best contribute by doing what they simply do not have time to do. Shut out the noise from both recriminations about the past and emergencies of the present and focus on the immediate future (as opposed to the present which is already passed, or the more distant future a few months away, for which there will be plenty of time to observe before orienting and there is no point in speculating).
While Four Corners twitters about “test, test, test”, the need to enforce quarantine on all returning travellers and to rapidly expand intensive care and other hospital capacity, it is safe to assume the public health authorities are already acting on all those:
- The test kits, masks, alcoholic sanitzers etc that should have been stockpiled long before advance notice was available are now being ramped up as fast as they can.
- Strict enforcement of quarantine at the borders by actually escorting arrivals into secure accommodation that should have been started long ago is now being done.
- The public information campaigns on hygiene and “social distancing” which should have begun much earlier have now got to the point where they do have the full attention of nearly the entire population. The enforcement of prohibiting gatherings of more than two people is sufficient to ensure that.
- Follow ups for organizing delivery services to replace shopping, contact with individuals and households in distress and homeless people etc etc are being rolled out with whatever levels of bumbling are unavoidable. This will be done like grocery and pharmaceutical supply chain issues at achievable linear rates that will not significantly add to the level of the impending health catastrophe.
- But the danger of catastrophe remains because no matter how brilliantly the expansion of hospital facilities for severe cases, Intensive Care Units for the most severe and ventilators for the ICUs are ramped up, they will still be overwhelmed unless other interventions actually reduce the “R” multiple from infections to new infections below 1 very soon.
Enquires into what could have been done better in the past (and accountability) will be important for the long term in which we can expect to be dealing with successive waves each time restrictions are lifted until an effective vaccine is deployed – expected to take 12-18 months.
But right now, the focus must be entirely on the immediate future for the first peak, which is only weeks away. What additional measures that are NOT already being taken can still be taken to push the rate R below 1? Others can and should come up with other such lower priority measures. Here’s my list.
What Must be Done Now
1. Announce that separate accommodation for everybody infected will be made available so that a lower proportion of the rest of their household remaining in enforced self-isolation will actually become infected and thus further reduce the overall transmission rate in addition to the higher priority measures already undertaken.
2. Announce that separate accommodation for everybody particularly vulnerable who is currently living with people less vulnerable will be made available to directly reduce the mortality rate among those vulnerable people.
3. Announce that these and related initiatives for homeless etc will take time to roll out and will initially be available only to those who need it most urgently as coordinated with the “package” for maintaining contact and mental health well-being etc.
4. Announce that preliminary estimates indicate subsantial numbers of premises previously used for other purposes and substantial numbers of people not currently working on other activities will be needed both to deploy and then to staff this emergency accommodation for the large case loads expected and registrations to participate in this new sector of the economy will be opened shortly.
5. Implement the long overdue announcements. But first announce them to pave the way for clamour rather than resentment.
PS
Apologies for both delay and haste. After having had to make a trip to the city to replace my phone after intending to be in isolation I had to make another trip out to replace a computer and then another to replace the new phone. So I haven’t had time to write better and still won’t until after setting up computer. (This is composed on Android Tablet and while still not back on email).